Diabetic retinopathy is a common and serious complication of diabetes that can lead to significant vision loss and, in some cases, blindness.
This ocular condition affects the blood vessels of the retina, the thin membrane at the back of the eye that contains the photoreceptors.
In this article, discover the different forms of diabetic retinopathy, each with distinct characteristics and stages that can have a lasting impact on vision.
Non-proliferative diabetic retinopathy (NPDR)
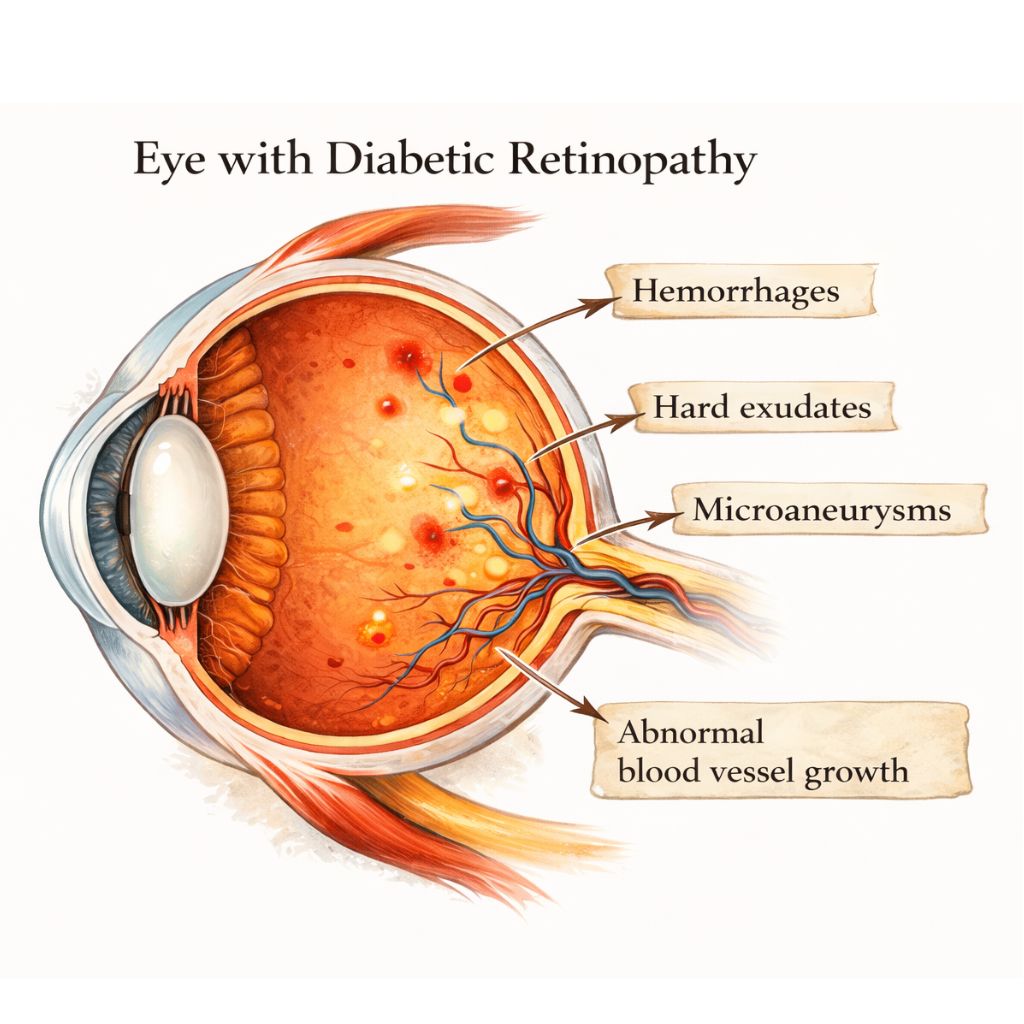
The earliest form of this eye disease is non-proliferative diabetic retinopathy (NPDR).
At this stage of diabetic retinopathy, structural changes affect the retinal blood vessels, including the formation of microaneurysms, small hemorrhages, and fluid leakage, resulting in retinal edema.
These retinal changes may lead to a reduction in visual acuity; however, patients frequently remain asymptomatic during the early stages, which complicates early diagnosis.
Proliferative diabetic retinopathy (PDR)
As the disease progresses, it may evolve into proliferative diabetic retinopathy (PDR).
This form of diabetic retinopathy is characterized by the growth of abnormal new blood vessels, a response to retinal ischemia caused by degeneration of the normal vasculature.
These new vessels are fragile and may cause vitreous hemorrhage, leading to a sudden decrease in central or peripheral vision. This proliferation can also abruptly restrict the patient’s visual field.
Diabetic maculopathy
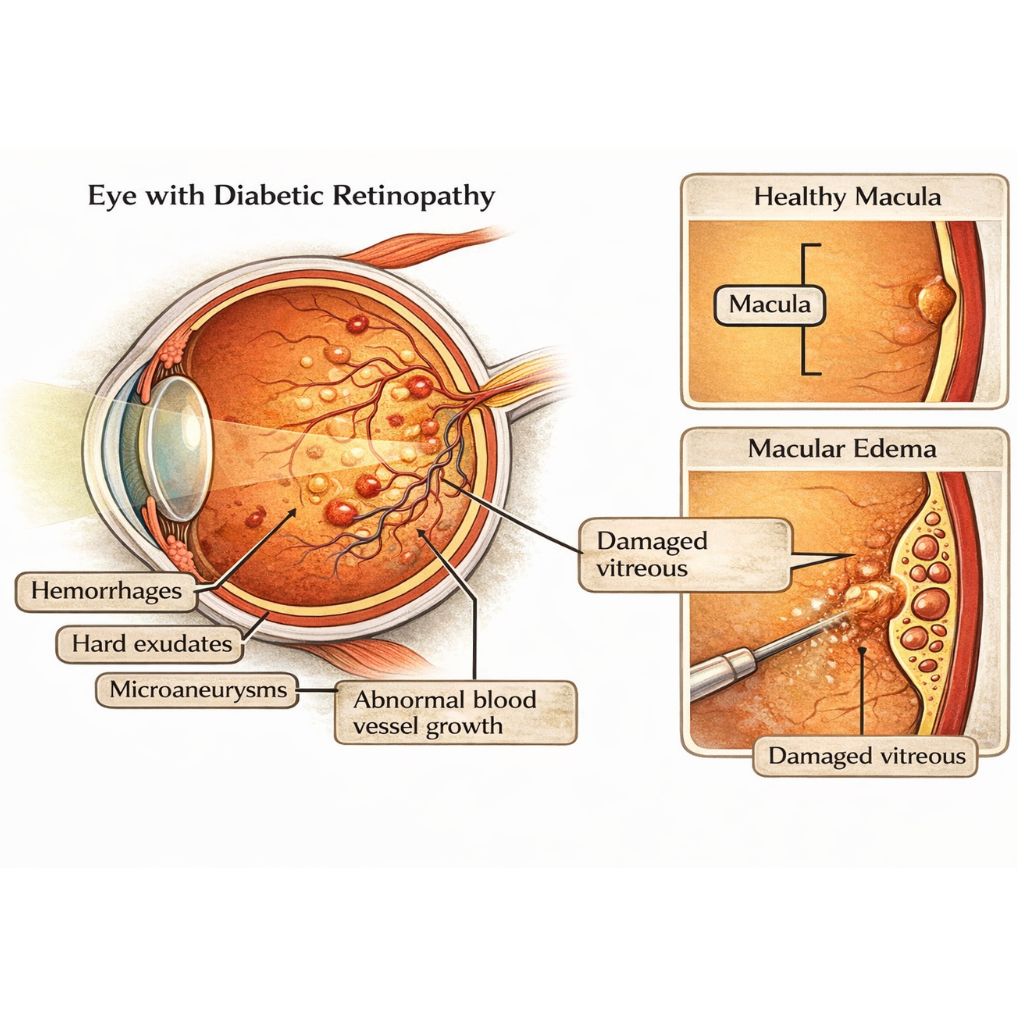
A major aspect of diabetic retinopathy is diabetic maculopathy, which affects the macula, the area of the retina responsible for sharp central vision.
Although its effects may resemble those of AMD (age-related macular degeneration), ophthalmologists clearly distinguish between these two conditions.
In the exudative form, abnormal vessel growth or capillary leakage leads to hemorrhages and loss of central vision.
In the atrophic form, there is a progressive destruction of the retinal pigment epithelium.
In both cases, patients experience significant difficulty reading or recognizing faces.
Diabetic macular edema
Diabetic macular edema is caused by the accumulation of blood and fluid within the retina due to damaged retinal capillaries.
As fluid builds up, the retina thickens (swells), and vision in the affected area becomes impaired.
When the macula is involved, central vision is severely reduced.
Macular involvement may occur independently of peripheral retinal damage but requires urgent management by an ophthalmologist.
The impact of blood pressure on retinal arteries
Monitoring arterial health is essential in diabetic patients. Poorly controlled blood pressure can worsen retinal damage.
This condition is known as associated hypertensive retinopathy, which causes vessel stiffening and accelerates fluid leakage. The combination of these vascular conditions makes diabetes management even more complex for the medical team.
Screening and ophthalmologic examination for diabetic retinopathy
Early screening for diabetic retinopathy is crucial, particularly in diabetic patients, as detection of early signs during regular ophthalmologic examinations helps slow disease progression.
To identify these abnormalities, specialists use tools such as fluorescein angiography and fundus examinations.
Treatment and rehabilitation of diabetic retinopathy
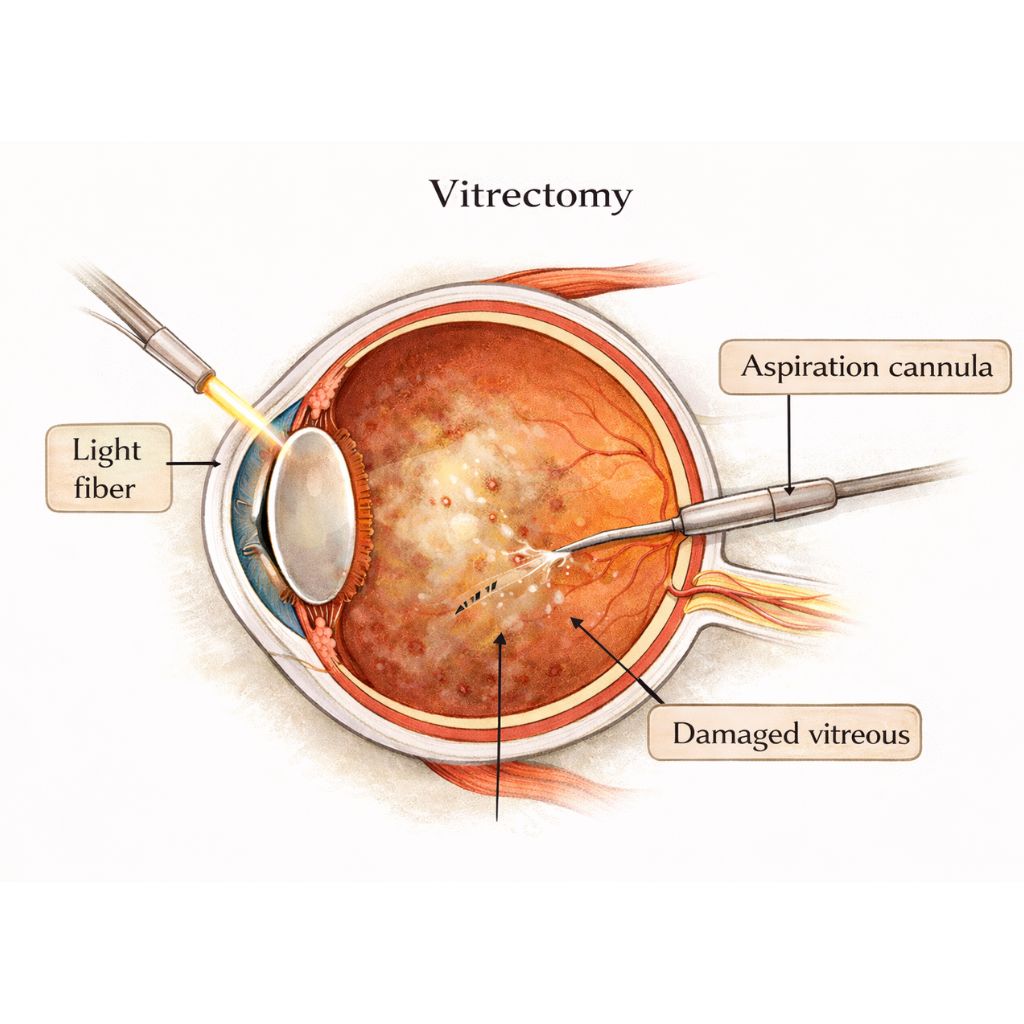
Surgical procedures, such as vitrectomy, may sometimes be necessary to remove hemorrhages or scar tissue.
As diabetic retinopathy remains the leading cause of severe visual impairment in adults, prevention is key.
For patients who have already experienced vision loss, visual rehabilitation (low-vision therapy) is essential to help them make the best use of their remaining peripheral vision and maintain daily independence.
To conclue
Diabetic retinopathy represents a serious threat to visual health. Vigilance, metabolic control, and annual ophthalmologic follow-up are the cornerstones of managing this condition. When addressed at the right time, it is possible to prevent irreversible vision deterioration.
Nous utilisons des cookies pour vous garantir la meilleure expérience sur notre site web. Si vous continuez à utiliser ce site, nous supposerons que vous en êtes satisfait.